LEARN: Breast cancer and HRT
The use of hormone replacement therapy (HRT) in individuals with a history of breast cancer is complex, as breast cancer is often hormone-sensitive, and there is concern that HRT could increase the risk of recurrence
Risk Assessment:
• Individualized Approach: Decisions should consider the type of breast cancer, time since diagnosis, other risk factors (e.g., BRCA mutations), and the severity of menopausal symptoms.
• Non-Hormonal Alternatives: First-line management typically includes non-hormonal treatments for menopausal symptoms, such as SSRIs/SNRIs, gabapentin, or cognitive behavioral therapy (CBT), to avoid potential risks.
HRT can be prescribed after breast cancer, but it depends on the individual and cannot be generalised. At FGP we try to prioritise appointment for wāhine and whānau who going through, or who have experienced breast cancer because we believe on supporting you as a whole person, and not defining you by your breast cancer.

Risk factors
A great infographic on the risk factors of breast cancer. It highlights that estrogen only HRT decreases the risk of breast cancer and drinking alcohol or being obese increase the risk of breast cancer. For me this is why taking HRT needs to be a personal decision, and put into perspective. If you feel so awful with hormonal related symptoms and you can't exercise (which decreases your risk of breast cancer!), this puts you at increased risk of drinking, weight gain and stress!

HRT and Breast Cancer
The Australasian Menopause Society (2019) provides an overview of the relationship between menopausal hormone therapy (MHT) and breast cancer risk. A key study by Beral et al. in The Lancet quantifies this risk, examining various forms of MHT, including estrogen-only and combined estrogen-progestogen therapies, across different durations and initiation times relative to menopause. The study found that combined MHT is associated with an 8.3% risk of breast cancer over 20 years, equating to a 1 in 12 chance. The article emphasizes the importance of balancing the benefits and harms of MHT, suggesting that clinicians should assess patients holistically, considering personal and family histories, as well as individual concerns during the menopause transition.

Breast cancer and menopause
The Australasian Menopause Society provides an information sheet exploring the connection between breast cancer and menopause, particularly in the context of menopausal hormone therapy (MHT). Here are the key points:
Duration and Timing: The risk rises with longer use of MHT and decreases after stopping it. Starting MHT close to menopause may have a different risk profile compared to starting it years later.
Other Risk Factors: Non-hormonal factors such as obesity, alcohol use, and lack of physical activity also contribute to breast cancer risk, emphasizing the need for a broader lifestyle approach.
Individualized Approach: Decisions around MHT should be tailored, taking into account personal risk factors, family history, and individual health needs.
The information also emphasizes the importance of breast health awareness, routine screening, and discussing alternative treatments. For women who may not find MHT suitable, there are other effective options available for managing menopause symptoms, including non-hormonal therapies and lifestyle modifications.
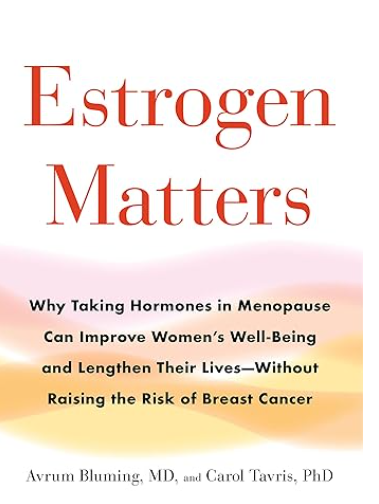
Estrogen Matters
A book all about the role of estrogen and why breast cancer is not just about estrogen.
This is a fantastic, comprehensive, evidenced based book, told my an inspiring, progressive clinician who has fought, and continues to fight to enable women access to what enables them to live their best lives.
Listen: Breast cancer and hormones
A must-listen for those who are concerned about breast cancer and whether to take estrogen.
The history of HRT has been clouded by misinformation, and sadly, many people, including healthcare professionals, still harbor fears about it. When I prescribe HRT, I want my patients to feel confident that it’s the right choice for them, especially since they are often told by others, 'You need to stop that; it will give you breast cancer'
We need to dispel these myths!